
Don't Play It by Ear: Appropriate Antibiotic Prescribing in Acute Otitis Media
Ashleah Courtney, MD, MSPH, FAAP
Acute otitis media is the leading reason pediatricians prescribe antibiotics — and a leading opportunity for antibiotic stewardship. Many AOM diagnoses can be safely managed with watchful waiting, and when antibiotics are warranted, choosing the right drug, dose, and duration matters more than ever in the face of growing resistance. This clinical reference, prepared for the LA AAP's Red Stick Potpourri 2022 conference, walks Louisiana pediatricians through the current AAP guideline criteria for AOM diagnosis, when to observe versus treat, first-line and penicillin-allergy alternatives, and shorter-course prescribing supported by recent evidence.

Pediatrics from the Parishes
A Conference Reimagined
August 13 - 16, 2026
The Roosevelt Hotel • New Orleans, LA
Appropriate Antibiotic Prescribing in Acute Otitis Media
Acute otitis media (AOM) is the most common reason children receive antibiotics. Getting the drug, dose, formulation, and duration right is one of the highest-impact targets for outpatient antimicrobial stewardship in pediatrics.
On this page
Why acute otitis media matters for stewardship
AOM is the single most common indication for antibiotics in pediatrics. Roughly five million children are diagnosed each year, accounting for about ten million antibiotic prescriptions annually. By one year of age, 23% of children have experienced at least one episode; by age three, that figure reaches 60%.
Because the volume is so large, even small improvements in prescribing — the right drug, the right duration, and the right formulation — add up to a meaningful reduction in unnecessary broad-spectrum antibiotic exposure across a population. Those three choices together are what define good antibiotic stewardship for this condition.
Who should be diagnosed with AOM
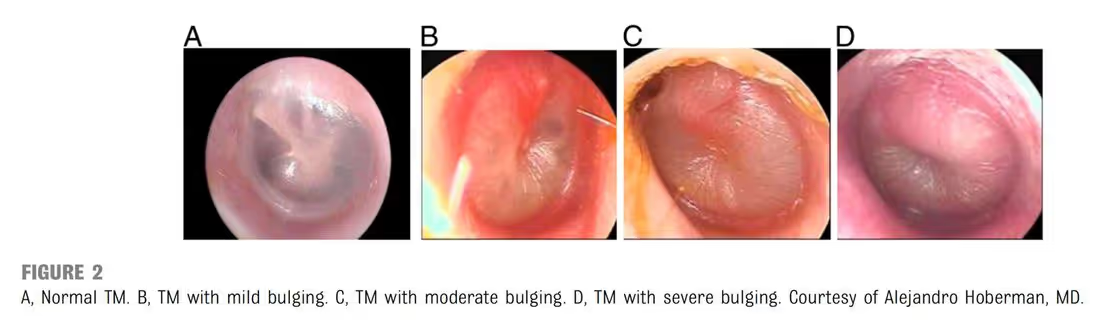
AOM should be diagnosed in children who have:
- Moderate to severe bulging of the tympanic membrane (TM), or new-onset otorrhea not attributable to acute otitis externa; or
- Mild bulging of the TM and recent (<48 hours) onset of ear pain — in a nonverbal child this may appear as holding, tugging, or rubbing the ear — or intense erythema of the TM.
AOM should not be diagnosed in children without a middle ear effusion (MEE), assessed by pneumatic otoscopy and/or tympanometry.
Examination findings and their test characteristics
| Finding | Sensitivity | Specificity |
|---|---|---|
| TM immobility | 95% | 85% |
| Cloudiness | 74% | 93% |
| Bulging | 50% | 97% |
Treat with antibiotics, or observe?
Who should receive antibiotics
- Children >6 months with severe signs or symptoms — moderate or severe otalgia, otalgia for at least 48 hours, or temperature ≥39 °C (102.2 °F).
- Children 6–23 months with bilateral AOM, even without severe signs or symptoms.
Who can be observed with close follow-up
- Children 6–23 months with unilateral AOM without severe signs or symptoms.
- Children ≥24 months with bilateral or unilateral AOM without severe signs or symptoms.
The observation option
Observation requires a reliable mechanism for follow-up and a way to begin antibiotics if the child fails to improve or worsens within 48–72 hours. It is a shared decision with the caregiver, not simply withholding treatment.
What to prescribe — and for how long
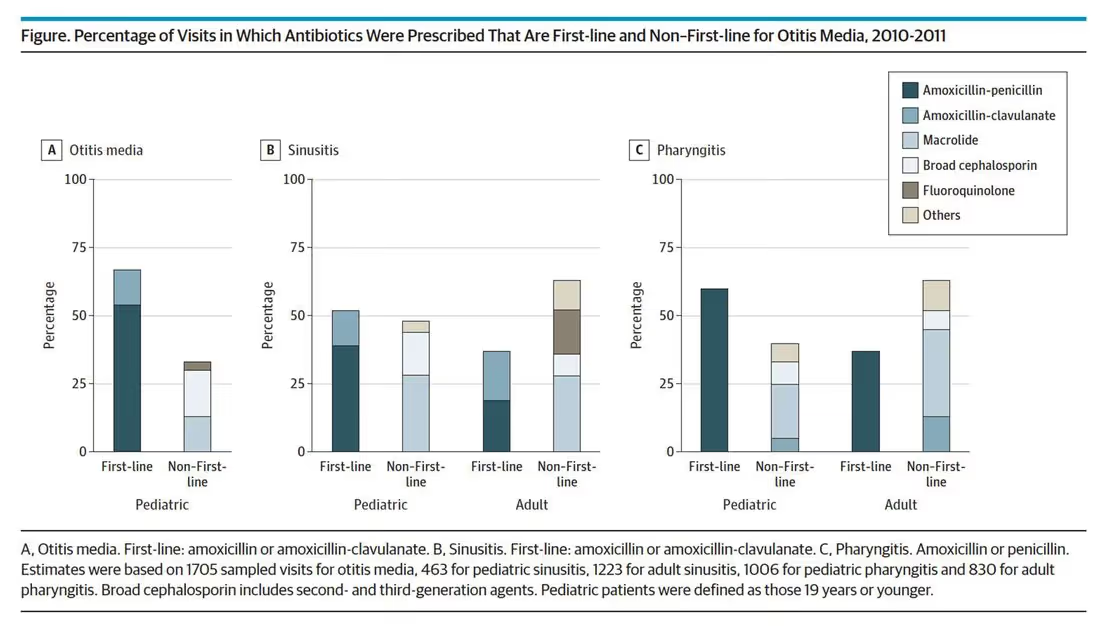
Choosing the drug
Amoxicillin is first-line when the child:
- Has not received amoxicillin in the past 30 days,
- Does not have concurrent purulent conjunctivitis, and
- Is not allergic to penicillin.
An agent with additional β-lactamase coverage (amoxicillin-clavulanate) is preferred when the child:
- Has received amoxicillin in the last 30 days,
- Has concurrent purulent conjunctivitis, or
- Has a history of recurrent AOM unresponsive to amoxicillin.
Choosing the duration
| Age | Duration | Notes |
|---|---|---|
| <2 years | 10 days | Multiple studies support longer durations in this age group. |
| 2–5 years | 7 days (AAP) | Some institutional guidelines use 5 days; no head-to-head 5- vs. 7-day comparison exists. |
| 6–12 years | 5 days | — |
A changing epidemiology
Both diagnoses and prescriptions for AOM have declined over the past several decades, in large part due to pneumococcal conjugate vaccination:
| Measure | 1995–1996 | 2005–2006 |
|---|---|---|
| Diagnoses | 950 | 634 |
| Prescriptions | 760 | 484 |
The mix of causative organisms has also shifted. After the introduction of PCV7 and PCV13, the share of AOM caused by Streptococcus pneumoniae fell, while Haemophilus influenzae and Moraxella catarrhalis became relatively more prominent.
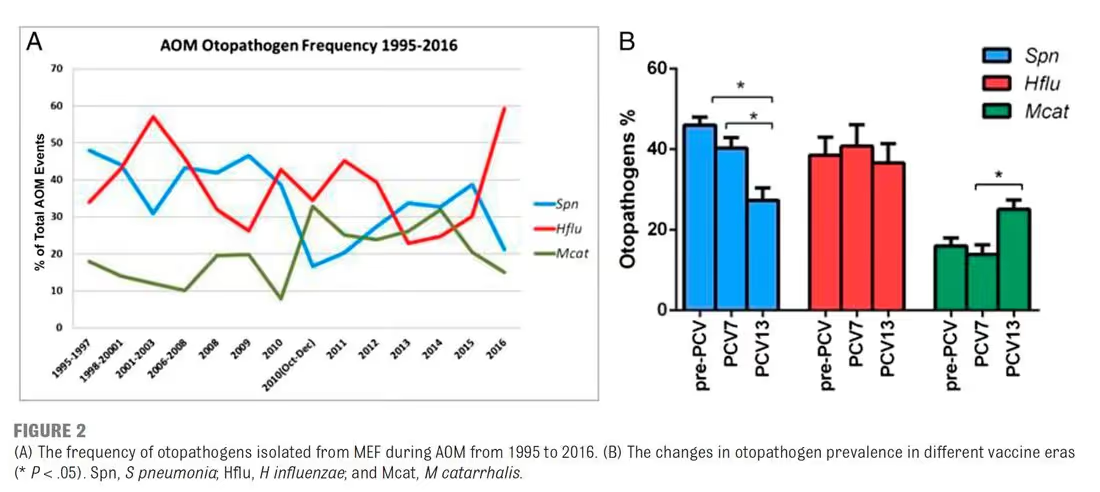
Why this raises the number needed to treat
S. pneumoniae is the otopathogen that benefits most from antibiotic treatment, because it is least likely to resolve on its own. As pneumococcus becomes a smaller share of cases — and as more episodes are viral or caused by organisms with higher spontaneous resolution — the number of children who must be treated for one to benefit continues to rise.
Resistance mechanisms and the high-dose rationale
The two dominant resistance mechanisms call for two different solutions:
| Organism(s) | Mechanism | Solution |
|---|---|---|
| S. pneumoniae | Alteration of the penicillin-binding protein, reducing β-lactam affinity | Overwhelm the protein with high-dose amoxicillin |
| H. influenzae, M. catarrhalis | Production of β-lactamase enzymes | Add a β-lactamase inhibitor (clavulanate) |
Because pneumococcal resistance is overcome by concentration rather than by a different drug, the answer for S. pneumoniae is more amoxicillin — not a switch to a broader agent.
The trouble with amoxicillin-clavulanate
Amoxicillin-clavulanate comes in many formulations with different ratios of amoxicillin to clavulanate. For pneumococcal coverage we want a high amoxicillin dose, which means favoring a high amoxicillin-to-clavulanate ratio. The highest available is the ES suspension at 14:1.
The clavulanate problem
If a lower-ratio (non-ES) formulation is pushed to "high-dose" amoxicillin, the child receives excess clavulanate, which causes diarrhea. This is associated with worse caregiver-reported quality of life and, downstream, avoidance of amoxicillin-clavulanate altogether — driving clinicians toward oral third-generation cephalosporins that are poorer choices.
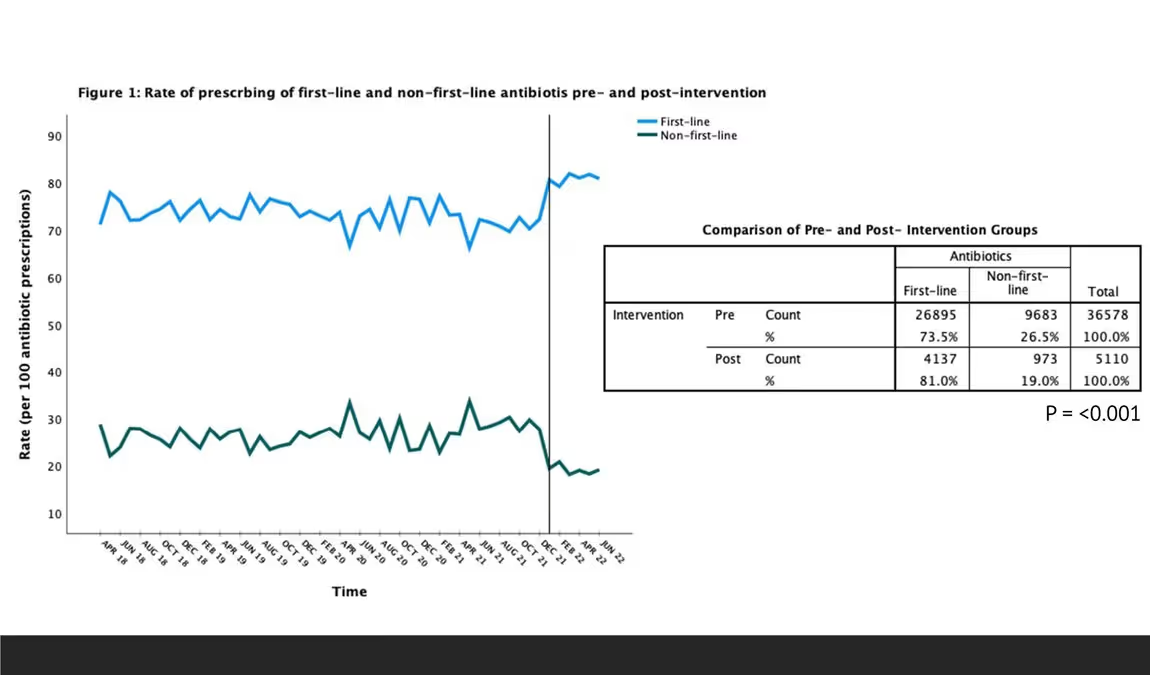
A practical fix is a clinical decision support tool that maps the AOM indication directly to the correct high-ratio ES formulation, so the prescriber doesn't have to navigate the formulary list manually. In one implementation, this kind of order-entry support produced a 29% increase in selection of the recommended formulation (P<0.01), with a smaller, non-significant change in dose selection.
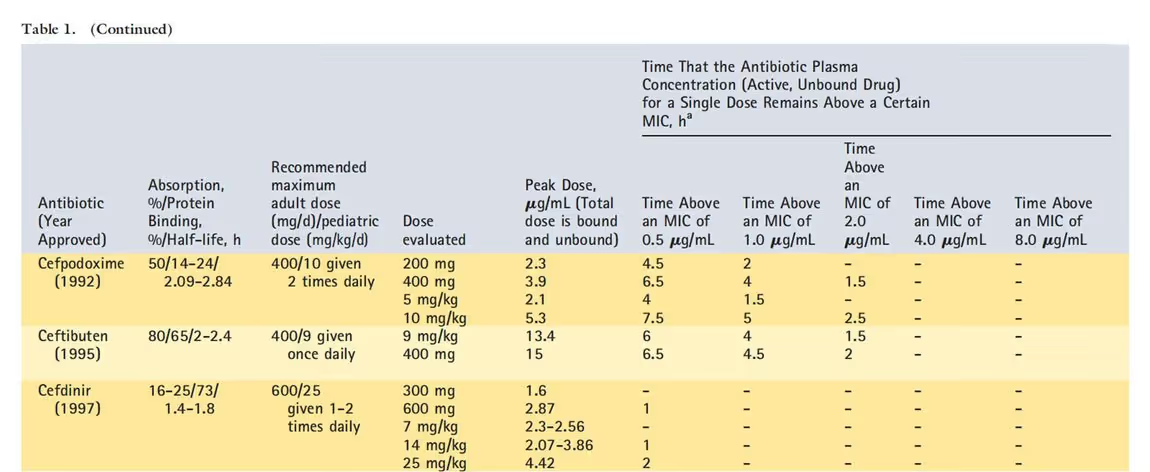
Why not a third-generation cephalosporin?
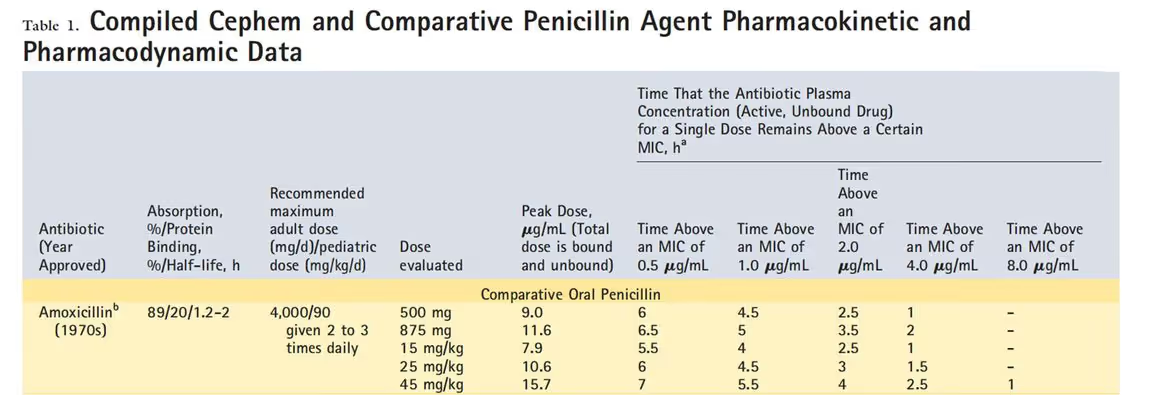
Cefdinir is attractive for its once-daily dosing and palatability, and is often marketed on the strength of non-inferiority trials. But it has real pharmacologic limitations: poor absorption, a short half-life, and high protein binding. Pneumococcal serotype 19A in particular shows high resistance, and cefdinir is associated with higher rates of community-acquired Clostridioides difficile infection than first-line agents.
A pharmacodynamic caution: do not extrapolate susceptibility
For β-lactams, S. pneumoniae susceptibility can be tested directly or extrapolated from penicillin testing — but the breakpoints differ dramatically by drug. Amoxicillin susceptibility is extrapolated from a penicillin MIC ≤2, whereas cefdinir requires a penicillin MIC ≤0.06. The practical result is that far fewer isolates are covered by cefdinir than by amoxicillin or ceftriaxone.
| Drug | MIC determination | Susceptible isolates |
|---|---|---|
| Amoxicillin | Penicillin MIC ≤2 | 94% |
| Cefdinir | Penicillin MIC ≤0.06 | 44% |
| Ceftriaxone | MIC ≤1 | 99% |
Key teaching point
Ceftriaxone susceptibility (99%) cannot be used to predict cefdinir susceptibility (44%). They are not interchangeable. Cefdinir's role should be limited to penicillin-allergic patients.
Outpatient stewardship in practice
Many familiar stewardship tactics — prospective audit and feedback, "handshake" rounds, formulary restriction — were designed for the inpatient setting. The challenge is translating them into something feasible in a busy outpatient clinic.
CDC Core Elements of Outpatient Antibiotic Stewardship
The CDC's 2016 framework defines four core elements:
- Commitment — demonstrate dedication to and accountability for optimizing prescribing and patient safety.
- Action for policy and practice — implement at least one policy or practice to improve prescribing, assess whether it works, and modify as needed.
- Tracking and reporting — monitor prescribing and provide regular feedback, or have clinicians self-assess.
- Education and expertise — provide educational resources to clinicians and patients and ensure access to stewardship expertise.
The Joint Commission's R3 Report extended antimicrobial stewardship requirements to accredited ambulatory health care organizations effective January 1, 2020, through new elements of performance in the Medication Management chapter (Standard MM.09.01.03) — including naming a stewardship leader, setting an annual goal, implementing evidence-based guidelines, educating staff, and collecting and reporting data.
What a feasible outpatient intervention looks like
Embedding guideline-concordant choices into order entry — a SmartSet that defaults to high-ratio ES amoxicillin-clavulanate for AOM, plus an advisory that fires when cefdinir is selected for AOM, sinusitis, or pharyngitis — combines the "action," "tracking," and "education" elements at the point of care without adding clinic workflow.
Take-home points
- As the most common indication for antibiotics in pediatrics, AOM is an excellent target for improving prescribing practices.
- With a high incidence of viral pathogens and a falling prevalence of S. pneumoniae in the post-vaccine era, the number needed to treat for AOM is rising.
- For pneumococcus, the answer is more amoxicillin (high-dose), not a broader drug; for β-lactamase producers, add clavulanate using a high-ratio ES formulation to minimize diarrhea.
- Cefdinir susceptibility cannot be extrapolated from ceftriaxone susceptibility. Cefdinir's role should be limited to penicillin-allergic patients.
Sources & further reading
- American Academy of Pediatrics. The Diagnosis and Management of Acute Otitis Media. Pediatric Clinical Practice Guidelines & Policies, 21st ed., 2021:391–428.
- Kaur R, Morris M, Pichichero ME. Epidemiology of acute otitis media in the postpneumococcal conjugate vaccine era. Pediatrics. 2017;140(3):e20170181.
- Hersh AL, Fleming-Dutra KE, Shapiro DJ, Hyun DY, Hicks LA. Frequency of first-line antibiotic selection among US ambulatory care visits for otitis media, sinusitis, and pharyngitis. JAMA Intern Med. 2016;176(12):1870.
- Parker S, Mitchell M, Child J. Cephem antibiotics: wise use today preserves cure for tomorrow. Pediatrics in Review. 2013;34(11):510–524.
- Block SL, Schmier JK, Notario GF, et al. Efficacy, tolerability, and parent-reported outcomes for cefdinir vs. high-dose amoxicillin/clavulanate oral suspension for acute otitis media in young children. Curr Med Res Opin. 2006;22(9):1839–1847.
- Klein JO. Otitis media. Clin Infect Dis. 1994;19(5):823–833.
This page is an educational summary for healthcare professionals and does not replace the full clinical practice guideline or individual clinical judgment. Refer to current AAP guidance and product labeling for dosing, susceptibility, and population-specific recommendations. Adapted from a continuing education presentation by Ashleah Courtney, MD, MSPH, FAAP.