

Head Shape Evaluation in Infants and Young Children
A practical, exam-based approach to distinguishing benign positional head-shape changes from single-suture craniosynostosis — and knowing when, where, and how to refer.
Objectives
- Perform and document a systematic head-shape exam.
- Identify the classic head shapes for plagiocephaly and single-suture craniosynostosis.
- Recommend appropriate and timely treatment of common head-shape anomalies.
Normal Skull Anatomy and Growth
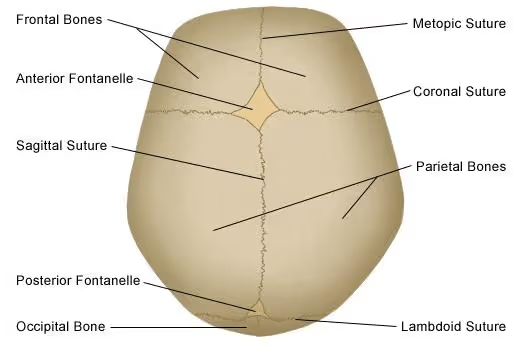
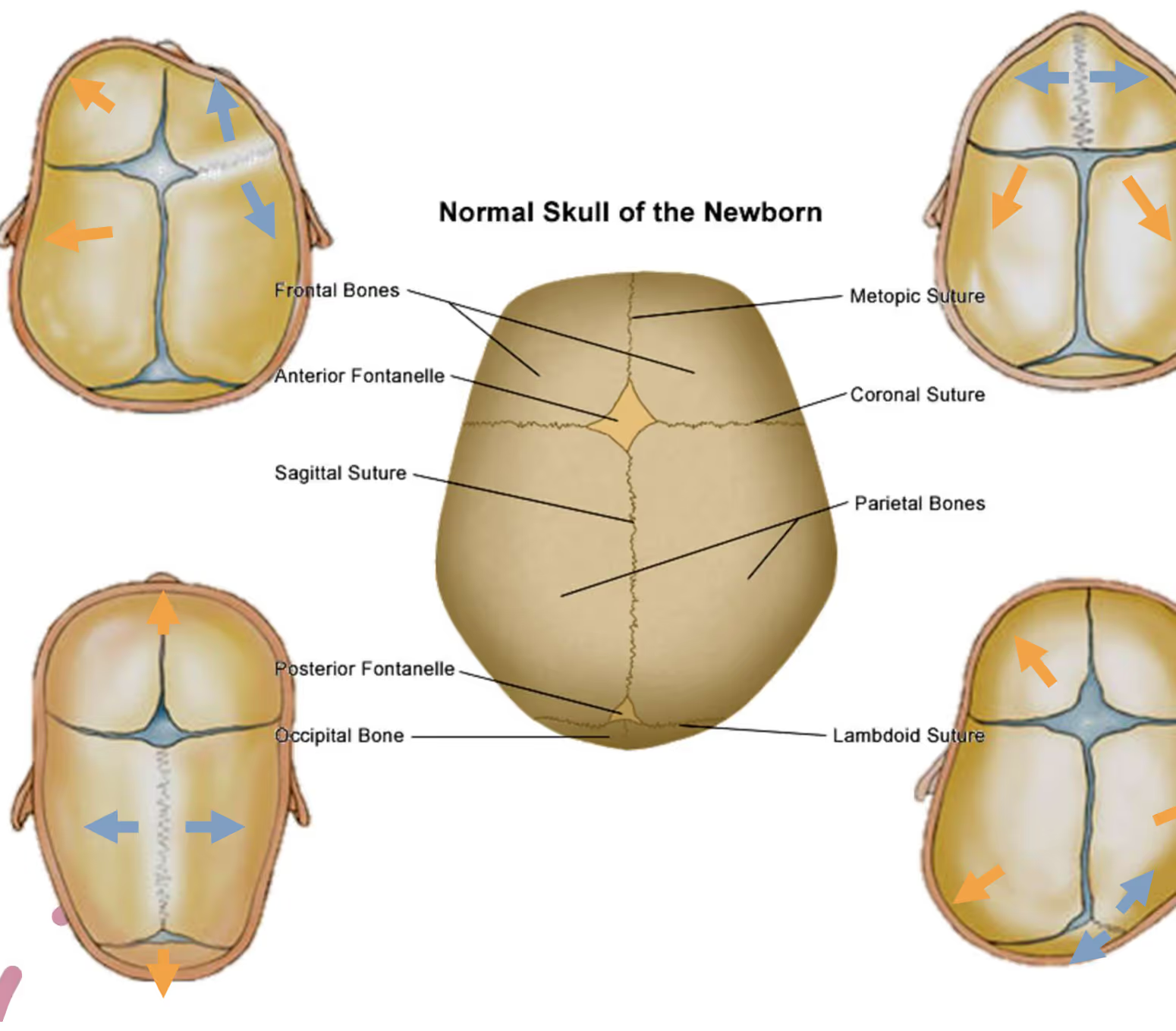
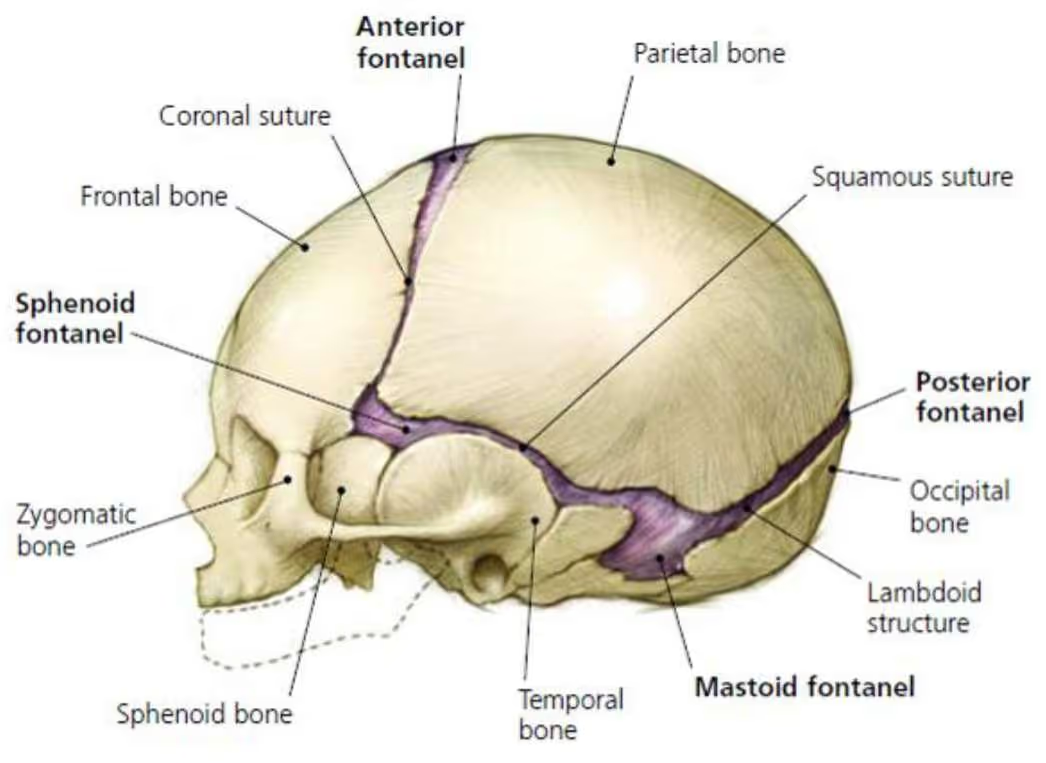
The infant skull is made of 5 major bones separated by 6 major sutures, with fontanelles at the suture junctions. The sutures allow the skull to deform during birth and to grow rapidly afterward. Skull growth is driven by the expanding brain and CSF volume — the brain triples in size by one year and reaches roughly 85% of adult size by age 3.
Normal Fontanelle and Suture Closure
Fontanelle timing
- Anterior fontanelle: typically closes around 9–15 months (range 3–26 months).
- Posterior fontanelle: typically closed by 2 months; can be hard to find in newborns.
A "closed" fontanelle simply means the soft spot is no longer palpable. It does not mean the sutures are fused, and it does not mean growth has stopped.
When closure timing matters
With normal head growth, head shape, and development, abnormal closure timing alone is not a reason to worry about craniosynostosis. However, closure timing can be a clue to other conditions:
Early closure / small fontanelle
- Hyperthyroidism
- Hyperparathyroidism
- Hypophosphatasia
- Rickets
Delayed closure / large fontanelle
- Hypothyroidism
- Malnutrition
- Trisomy 21
- Hydrocephalus
Normal suture closure ages
- Metopic: 3–9 months (sometimes as early as 2 months). Commonly forms a palpable or visible ridge — a benign normal variant when the head shape is otherwise normal.
- Sagittal: ~22 years · Coronal: ~24 years · Lambdoid: ~26 years.
Craniosynostosis Overview
Craniosynostosis is the early fusion of one or more cranial sutures, typically occurring in utero, with an incidence of roughly 1:2,500 births. About 97% of cases involve a single suture; of those, ~85% are non-syndromic and 6–10% are familial.
Fused sutures carry an increased risk of elevated intracranial pressure (single-suture 4–42%, multi-suture 50–68%), language delay, learning disability (single-suture 10–30%), and other developmental delays — which is why timely identification matters.
Head-Shape History
Birth history — and why it matters
- Gestational age: premature infants have higher risk of deformational plagiocephaly/brachycephaly and of vitamin D deficiency.
- Route of delivery & reason for C-section: craniosynostosis is associated with a higher rate of unplanned C-section.
- Prenatal concerns (constraint, oligohydramnios, breech, multiples) and maternal health (diabetes, thyroid disease, tobacco use): intrauterine head constraint, twin-or-more pregnancy, maternal smoking, and maternal thyroid disease are all craniosynostosis risk factors.
- Breech molding can mimic sagittal craniosynostosis.
Specific head-shape questions — and why they matter
- Shape at birth and over time: craniosynostosis is present at birth and does not improve; typical newborn molding improves with time.
- When first noticed: plagiocephaly is not present at birth and may worsen or improve over time.
- Sleep position: typically dictates the side of plagiocephaly.
- Head tilt / torticollis: makes any head shape worse.
- Developmental history: delayed motor milestones increase the risk of plagiocephaly.
The Systematic Head-Shape Exam
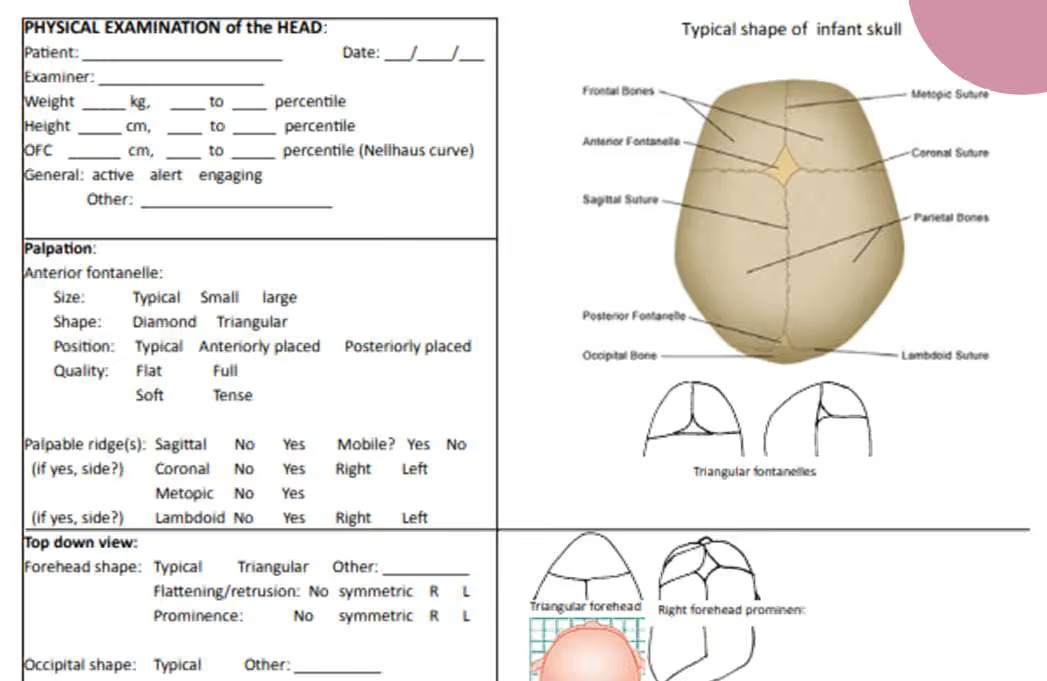
Work through the same sequence every time: palpation → top-down view → side view → posterior view (correcting for head tilt) → frontal/facial view. Begin with measurements.
Measurements
Record weight, height, and head-circumference percentiles; assess whether they are proportional and note who measured them.
Side-view findings to note
- AP diameter: typical, short, or long.
- Height: typical, turricephalic, tall forehead, or tall occiput.
- Prominence: prominent forehead and/or prominent occiput.
Single-Suture Craniosynostosis Patterns
Each fused suture produces a characteristic, reproducible shape. The table summarizes the hallmark findings; the sections that follow add the supporting detail.
| Suture | Overall shape | Hallmark findings | Approx. share / incidence |
|---|---|---|---|
| Sagittal | Narrow, elongated (long AP) | Relative macrocephaly; ridge over sagittal suture; widest point not bi-parietal (at/anterior to ears); prominent forehead & occiput | 40–50% (~1:4,200) |
| Metopic | Teardrop / triangular forehead | Ridge over metopic suture; bilateral forehead retrusion with visible lateral globes; bi-temporal constriction; narrow eye spacing; "small face on a big head" | 19–28% (~1:10,000) |
| Unicoronal | Rhomboid | Affected-side forehead swept back; ipsilateral eyebrow raised & eye opening larger; nasal tip twists away from defect; facial C-shape away from defect | 12–24% (0.7–1:10,000) |
| Lambdoid | Rhomboid (posterior) | Skull-base tilt; ipsilateral mastoid bulge; vertical ear dystopia (ear lower on affected side); contralateral parietal bulge | ~2% (0.1:10,000) |
Sagittal craniosynostosis
The most common single-suture form. Expect relative macrocephaly and a triangular anterior fontanelle in normal position (often larger than expected) with a non-mobile ridge over the sagittal suture. Top-down, the head is narrow and elongated with the widest point at or anterior to the ears rather than bi-parietal. The face is symmetric with a large forehead. Male:female ratio ~3.5:1. Treatment ages: endoscopic repair 1.5–4 months; open repair 4–8 months. Breech molding can mimic this pattern — history helps separate the two.
Metopic craniosynostosis
HC is normal to relatively macrocephalic with a small or closed anterior fontanelle and a ridge over the metopic suture. The forehead shows bilateral/symmetric retrusion with visible lateral globes, producing a teardrop shape with bi-temporal constriction, narrow eye spacing, and arched eyebrows. Male:female ~3.2:1; 25–30% are syndrome-associated. Treatment: endoscopic 1.5–4 months; open repair 9–14 months.
Unicoronal craniosynostosis
HC is more often normal. The anterior fontanelle is triangular (blunted toward the fused side) with a possible ridge over the affected coronal suture. The affected forehead is swept back (rhomboid shape, widest point askew temporal-to-parietal); the eyebrow is raised and the eye opening larger on the affected side, with the nasal tip and facial twist away from the defect. Male:female ~1:3.6; ~30% carry an FGFR3 or TWIST1 mutation, sometimes with C-spine changes. Treatment: endoscopic 1.5–4 months (less common); open repair 9–14 months.
Lambdoid craniosynostosis
The rarest single-suture form (~2% of cases) and the one most often confused with positional plagiocephaly. Look for the four hallmarks: skull-base tilt, ipsilateral mastoid bulge, vertical ear dystopia, and contralateral parietal bulge. The posterior view (corrected for head tilt) is key — the skull base is lower on the affected side with the ear lower on that side. Treatment: endoscopic 1.5–4 months (less common); open repair 9–14 months.
Positional Plagiocephaly and Brachycephaly
Positional (deformational) plagiocephaly is common — affecting roughly 22% of 2–6 month-olds (some studies approach 50%), with a male:female ratio ~1.5:1. It is acquired in the first 4–12 weeks, with flattening on the side the baby sleeps on, and ~20% have some degree of torticollis.
Plagiocephaly (positional)
- Normal HC.
- Parallelogram shape; same-side occipital flattening with slight same-side forehead prominence.
- Widest point still bi-parietal; ear shifted anterior on the affected side.
- Posterior view (tilt-corrected): skull base level, no mastoid bulge, ears symmetric vertically.
- Face generally symmetric; no nasal twist.
Brachycephaly (positional)
- Symmetric posterior flattening with occipital lift.
- Common in NICU babies (prolonged sedation/intubation).
- Increased risk with hypotonia or developmental delay.
- Plagiocephaly correlates with poorer cognitive outcomes.
Treatment of Positional Deformities
Conservative management (first line)
- Increased supervised tummy time and core strengthening.
- Less time on the back; repositioning in the crib/bed.
- Physical therapy for torticollis — refer early.
- PM&R referral if not improving.
Helmet therapy — what the evidence shows
Cranial orthoses are hard shells with foam lining that redirect skull growth, fitting closely in some areas and leaving room in flattened areas. They only "work" for asymmetric plagiocephaly — not brachycephaly — and are generally started at 4–6 months (and won't work if started after ~8 months), worn ~23 hours/day for 4–6 months at a cost of roughly $2,000–$2,500, often not covered by insurance unless asymmetry is significant.
What to Do With a Misshapen Head
If plagiocephaly is likely
- Conservative management.
- Refer to the Plagiocephaly Clinic (PM&R, Plastic Surgery, or Craniofacial Peds).
- Refer ASAP if significant asymmetry or torticollis — ideally no later than 6 months.
If craniosynostosis is suspected
- Refer to the Craniosynostosis Clinic (Neurosurgery, Plastic Surgery, or Craniofacial Peds).
- Call the Craniofacial Center to coordinate.
- Don't order imaging first — let the clinic guide work-up.
Children's Hospital of New Orleans — Craniofacial Center
To discuss a patient or coordinate a referral:
504.896.9857When referring for a suspected positional deformity, include standardized photos: face, left side, right side, top of head, and back of head — hair moved away from the ears, solid background, camera level with the floor, head centered and filling the frame.
References & Further Reading
- Dias MS, Samson T, Rizk EB, Governale LS, Richtsmeier JT; Section on Neurologic Surgery, Section on Plastic and Reconstructive Surgery. Identifying the Misshapen Head: Craniosynostosis and Related Disorders. Pediatrics. 2020;146(3):e2020015511. doi:10.1542/peds.2020-015511
- Dempsey RF, Monson LA, Maricevich RS, et al. Nonsyndromic Craniosynostosis. Clin Plast Surg. 2019;46(2):123–139. doi:10.1016/j.cps.2018.11.001
- Kiesler J, Ricer R. The abnormal fontanel. Am Fam Physician. 2003;67(12):2547–2552. PMID: 12825844
- Birgfeld CB, Saltzman BS, Hing AV, et al. Making the diagnosis: metopic ridge versus metopic craniosynostosis. J Craniofac Surg. 2013;24(1):178–185. doi:10.1097/SCS.0b013e31826683d1. PMID: 23348281
- Van Wijk RM, et al. Helmet therapy in infants with positional skull deformation: randomised controlled trial. BMJ. 2014;348:g2741.