

Spinal Dysraphism in Children: Types, Presentation, and Management
Spinal dysraphism describes a spectrum of congenital malformations of the spine and spinal cord, ranging from open neural tube defects such as myelomeningocele to subtle closed lesions that may present only with a cutaneous marker. Early recognition allows timely neurosurgical evaluation and helps preserve neurologic, urologic, and orthopaedic function.
Embryologic Origins
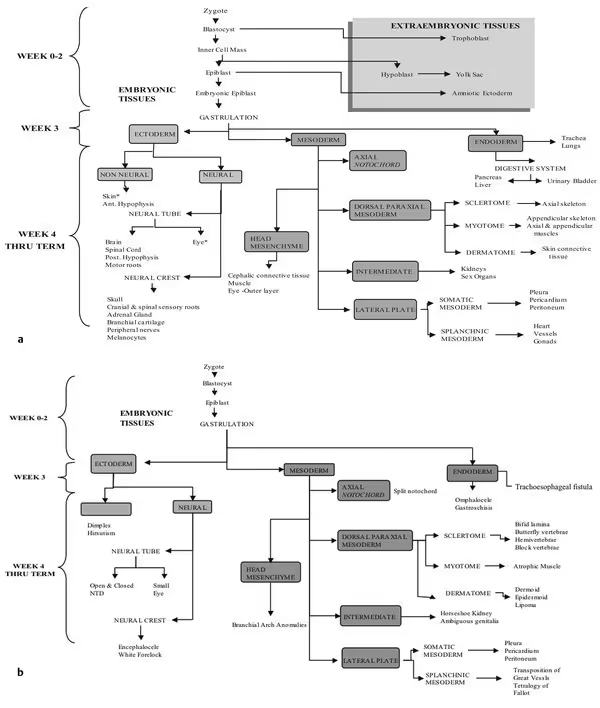
Spinal dysraphic states arise from errors during the formation of the embryonic nervous system. Open defects generally reflect a disturbance of primary neurulation (failure of the neural tube to close), while many closed lesions stem from abnormalities of secondary neurulation or premature disjunction of cutaneous and neural ectoderm. The flowchart below traces normal germ-layer development alongside the malformations that result when each step is disrupted.
Open Neural Tube Defects: Myelomeningocele
Myelomeningocele is the prototypical open neural tube defect and a defect of primary neurulation. It can be detected prenatally through an elevated maternal serum alpha-fetoprotein and acetylcholinesterase, and on prenatal ultrasound through two characteristic cranial findings.
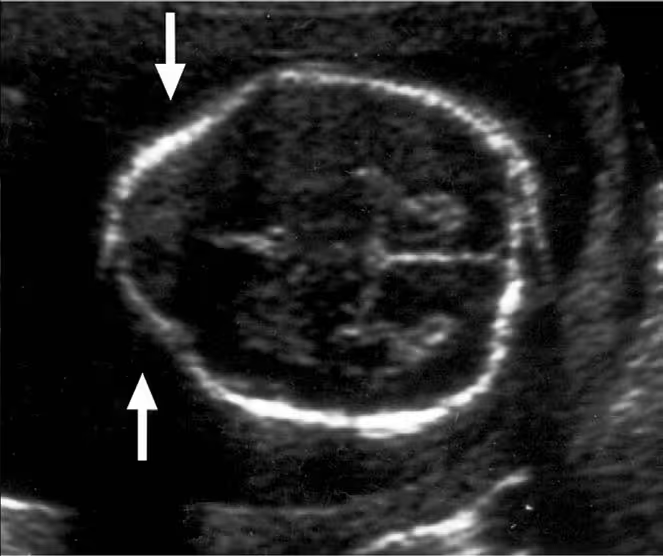
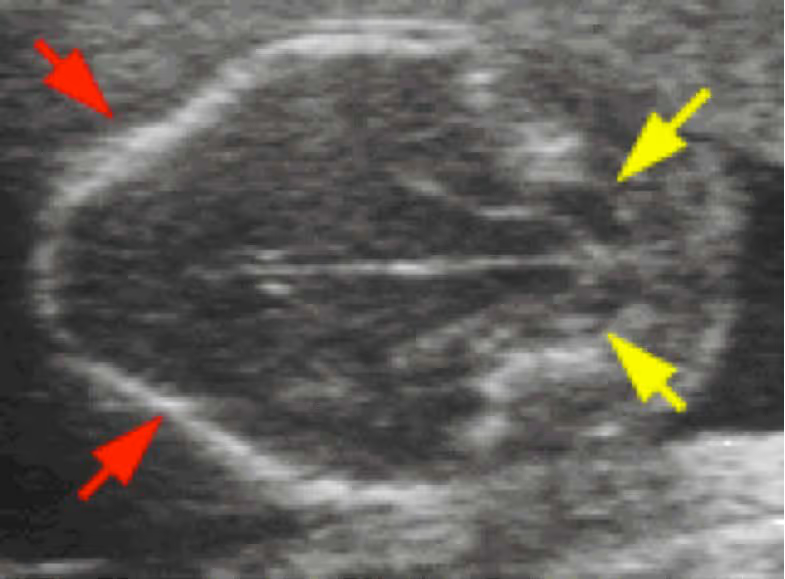
Prenatal ultrasound signs
- Lemon sign — scalloping of the frontal bones giving the fetal skull a lemon-like contour.
- Banana sign — abnormal anterior curvature of the cerebellum around the brainstem from hindbrain herniation.
Epidemiology and outcomes
Lifetime mortality is most often driven by the Chiari II malformation and by unrecognized shunt malfunction. The proportion of patients ultimately requiring a ventriculoperitoneal shunt (~60%) is notably lower than older reports approaching 80%.
Initial management of the newborn
- Surgical closure of the defect within 48–72 hours.
- Prophylactic antibiotic coverage (ampicillin and gentamicin).
- Head ultrasound, renal ultrasound, and spine radiograph (babygram).
- Keep the defect covered with a moist, non-adhesive dressing.
- Dedicated muscle-group testing to determine the affected neurologic level.
Three overarching phases guide care: initial stabilization and closure; assessment and treatment of hydrocephalus; and long-term management of shunt malfunction, Chiari II malformation, tethered cord, and syringomyelia.
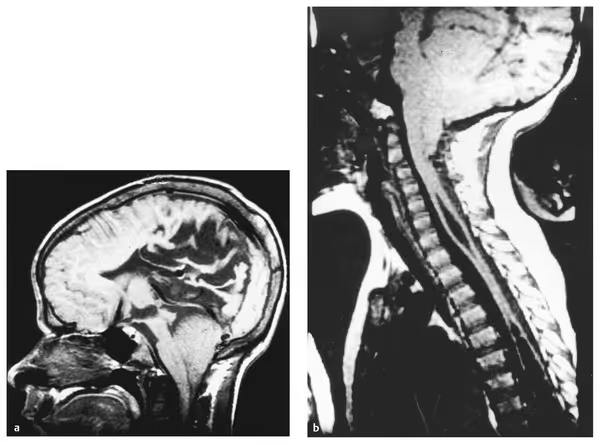
Chiari II malformation
Under the unified theory, Chiari II results from underdevelopment of the posterior fossa bone with crowding by the structures of the rhombencephalon. Herniation of the brainstem, cerebellar vermis, and fourth ventricle through the foramen magnum can produce lower cranial neuropathies, swallowing dysfunction, and disordered breathing.
Prenatal versus postnatal closure
A landmark randomized trial compared prenatal closure (before 26 weeks gestation, with delivery at 37 weeks) to standard postnatal repair. Prenatal surgery was associated with a decreased shunt rate and improved functional outcome, but with an increase in preterm labor. During counseling, caution is warranted when the ventricles measure 15 mm or larger, since prenatal surgery does not appear to improve outcome in that group.
Closed Neural Tube Defects
Closed (skin-covered) dysraphic lesions are easily missed in the newborn nursery because the spinal cord is not exposed. They are, however, frequently announced by cutaneous markers over the lower back.
Cutaneous markers
Cutaneous markers appear in roughly 3% of the general population, but in about 80% of patients with spinal dysraphism; two or more often coexist. They characteristically occur in the midline of the back, above the level of the coccyx, and commonly overlie the underlying spinal lesion. Examples include hairy patches (faun’s tail), dermal sinus openings, subcutaneous lipomas, skin tags or tails, capillary malformations, and atypical dimples.
When to suspect a closed defect
- Neurologic: lower-extremity weakness, muscle atrophy, radicular pain, abnormal gait.
- Orthopaedic: leg-length discrepancy, foot deformities.
- Urologic: recurring urinary tract infection, change or regression in continence.
Imaging
- MRI is the study of choice.
- Ultrasound can localize the conus in infants younger than 6 months, before posterior elements ossify.
- CT is a useful adjunct in lesions with bony abnormalities.
Meningocele
A meningocele is a congenital herniation of dura and arachnoid through a bony defect in the spine. Nerve roots may be involved, but the spinal cord typically is not. Incidence is approximately 0.3–0.4 per 1,000 births. Posterior meningoceles relate to secondary neurulation, whereas anterior meningoceles arise from mesenchymal abnormalities.

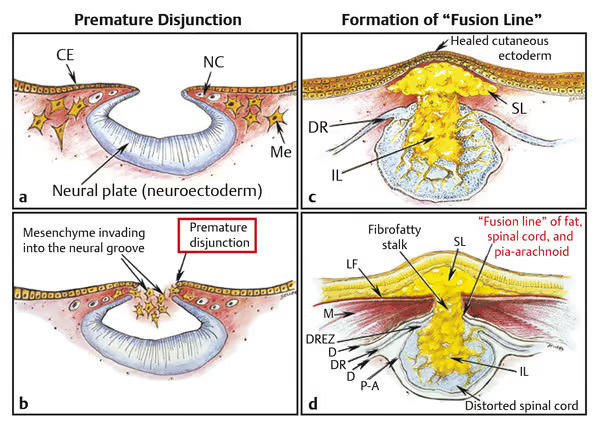
Spinal lipoma
Spinal lipomas form when cutaneous ectoderm separates prematurely from neural ectoderm (premature disjunction), allowing mesenchyme to enter the still-open neural groove and differentiate into fat that becomes incorporated into the cord.
Lipomas are classified by their relationship to the conus and cord:
- Dorsal: the lipoma–cord interface lies entirely on the dorsal surface of the lumbar cord, always sparing the distal conus.
- Terminal: the lipoma inserts into the caudal extremity of the conus without blending with the cord or its root entry zones.
- Transitional: the interface is undulating and tilted, sometimes rotating the placode toward a parasagittal orientation, but neural tissue remains ventral to the interface.
- Chaotic: the caudal portion lies ventral to the placode and engulfs neural tissue and nerve roots.

Two approaches to treatment exist: prophylactic surgery to prevent symptoms (commonly around 3 months of age, the more common approach in the United States), versus operating only once the patient becomes symptomatic (more common in Europe).
Dermal sinus tract
A dermal sinus tract occurs in approximately 1 in 2,500 births. Affected children are usually neurologically normal at birth, but the risk of neurologic deficit and infection rises with age if the tract is left untreated. Although there is no consensus on timing in uncomplicated, asymptomatic cases, surgery is reasonable once the infant is physiologically ready for the procedure.
Split cord malformation
Split cord malformations (historically termed diastematomyelia) divide the spinal cord into two hemicords and often present with an overlying faun’s tail. They are separated into two types:
- Type I: two hemicords separated by an osteocartilaginous median septum, each within its own dural sheath.
- Type II: two hemicords within a single dural envelope, separated by a fibrous septum.

Key Takeaways for the Pediatrician
- Open neural tube defects require closure within 48–72 hours and coordinated neurosurgical care.
- Midline lumbosacral cutaneous markers warrant a low threshold for spinal imaging, since most children with dysraphism display them.
- MRI is the imaging study of choice; ultrasound is useful before 6 months of age.
- New or progressive neurologic, orthopaedic, or urologic findings may signal a tethered cord and should prompt re-evaluation.
This page is an educational reference for clinicians and is not a substitute for individualized medical judgment or formal neurosurgical consultation. Adapted from a presentation by Jerome M. Volk III, M.D., LSUHSC New Orleans Department of Neurosurgery and Children’s Hospital of New Orleans.